

Background: Acute chest syndrome (ACS) frequently complicates sickle cell disease (SCD) and is a leading cause of hospitalization and mortality. Many factors have been implicated in ACS, including infections, thrombosis, fat and pulmonary emboli. However, a clear etiology is not defined in 50% of the cases and ACS is considered a clinical endpoint for different pathogenic processes (Vichinsky et al 2000). The non-specific nature of ACS makes diagnostic tests challenging, and there are no serum tests clinical used to aid diagnosis. Procalcitonin (PCT) is a prohormone of calcitonin and serum PCT rises within hours of an inflammatory stimulus. PCT has clinical utility as a marker of severe systemic inflammation, infection, and sepsis (Becker et al. 2008). Few studies have evaluated PCT as a biomarker for ACS in patients presenting with vaso-occlusive crises (VOC). Two studies have reported no difference in PCT (Biemond et al. 2018 and Stankovic et al 2011), while one study reported higher PCT between ACS and VOC (Patel et al 2014).
Methods: We retrospectively reviewed 106 patients with SCD who presented to the emergency department with fever and painful crises during 2015-2019. The patients were divided into two categories based on discharge diagnoses - patients with VOC only (n=88) and patients with ACS (n=18). Inclusion criteria for both groups were patients with SCD, 17 years and older and PCT measurement on presentation. Exclusion criteria were defined as patients who had received empiric antibiotics prior to PCT testing. Data collected on presentation included genotype, age, gender, complete blood count, PCT, creatinine, total bilirubin and hydroxyurea use. Length of stay was recorded. Data was analyzed between the two groups using descriptive statistics and accounting for unequal variances, withp-value set at 0.05 for significance.
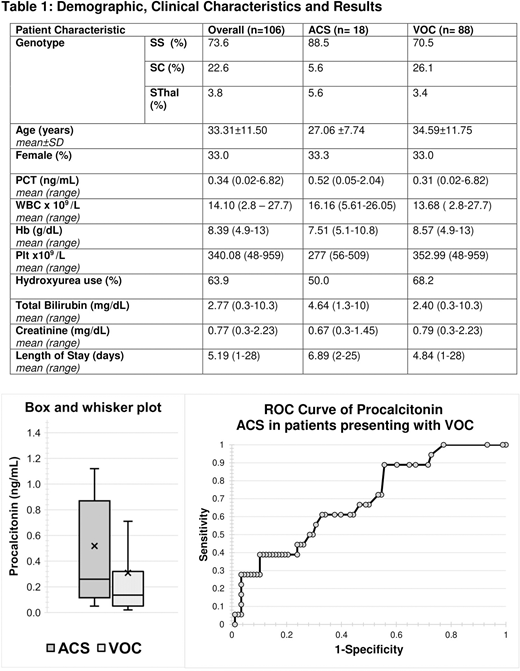
Results: Demographics and clinical characteristics are summarized in Table 1 (Figure). The sample included primarily adult males (77%), with about two-thirds on hydroxyurea. Genotype HbSS (73.6%) was most prevalent followed by HbSC (22.6%) and HbSβ (3.8%). The ACS group had a higher percentage of HbSS, lower use of hydroxyurea and higher mean bilirubin. Mean PCT for the ACS group was 0.52 ng/mL (range, 0.05-2.04), compared to 0.31 ng/mL (range, 0.02-6.82) in the VOC group; withp=0.084. ROC analysis showed a PCT>0.5ng/mL had 39% sensitivity and 85% specificity for ACS in this sample.
Conclusion: In this sample, PCT on presentation was higher in those with ACS compared to VOC, but this difference did not achieve statistical significance. Further study in a larger population would be useful to evaluate this finding.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal